Gluteal Region Anatomy
By : Omar M. Subhi Altaie• Definition
The buttocks or the Gluteal region is the prominent rounded area consisting of muscles and a thick layer of superficial fascia. It overlays the bony framework of the pelvis and distal end of the femur bone posterolaterally, superior to the thigh, it has several medical significance.
• Boundaries
Inferiorly : The lowest point of the buttocks is the Gluteal fold inferiorly, which separates it from the thigh.
Superiorly : The highest point is at the level of the Fourth lumbar spine which is the iliac crest of the bony framework of the pelvis, Superiorly separates the buttock from the back trunk.
In the middle : there is the Intergluteal cleft or natal cleft that separates one buttock from the other.
Laterally : it extends laterally to the posterior margin of the greater trochanter of the femur bone .
Superiorly : The highest point is at the level of the Fourth lumbar spine which is the iliac crest of the bony framework of the pelvis, Superiorly separates the buttock from the back trunk.
In the middle : there is the Intergluteal cleft or natal cleft that separates one buttock from the other.
Laterally : it extends laterally to the posterior margin of the greater trochanter of the femur bone .
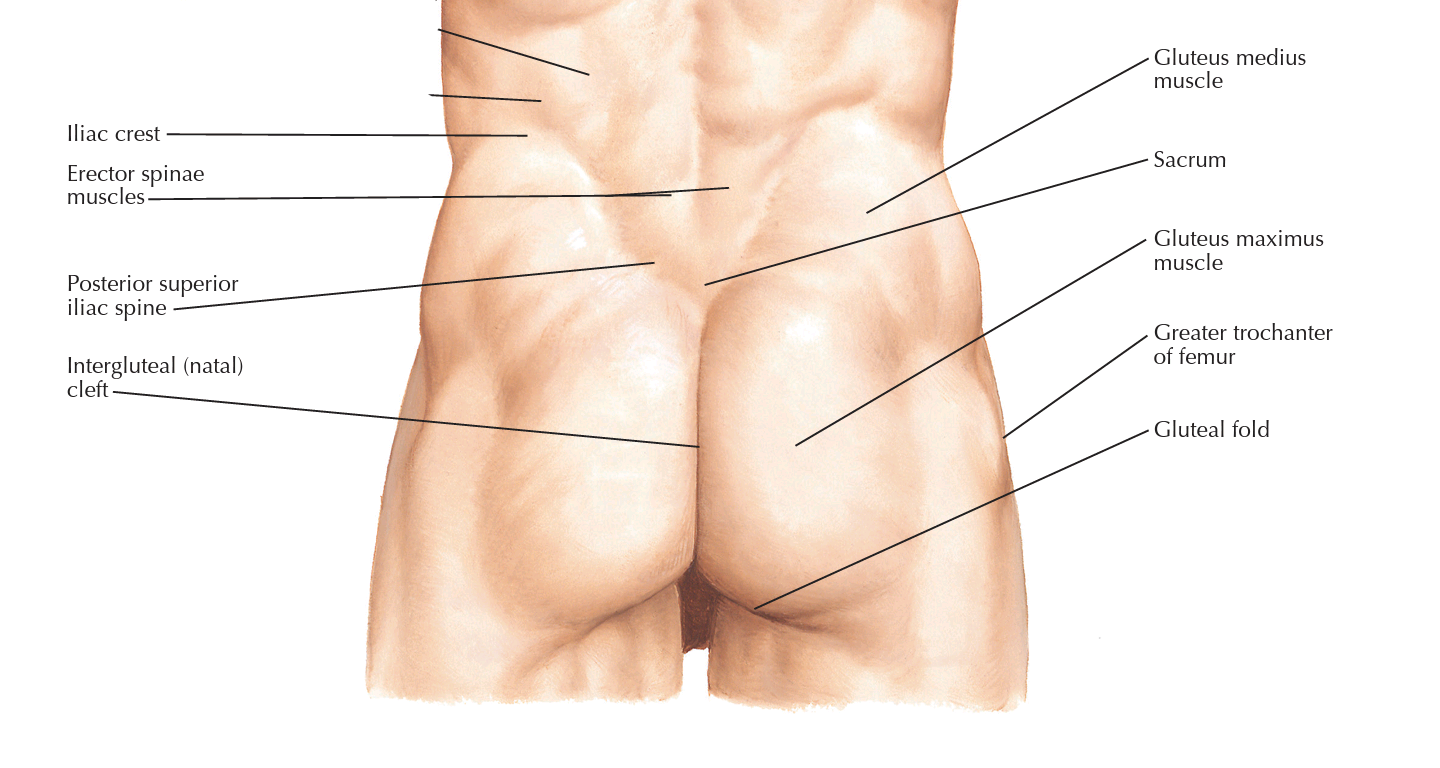
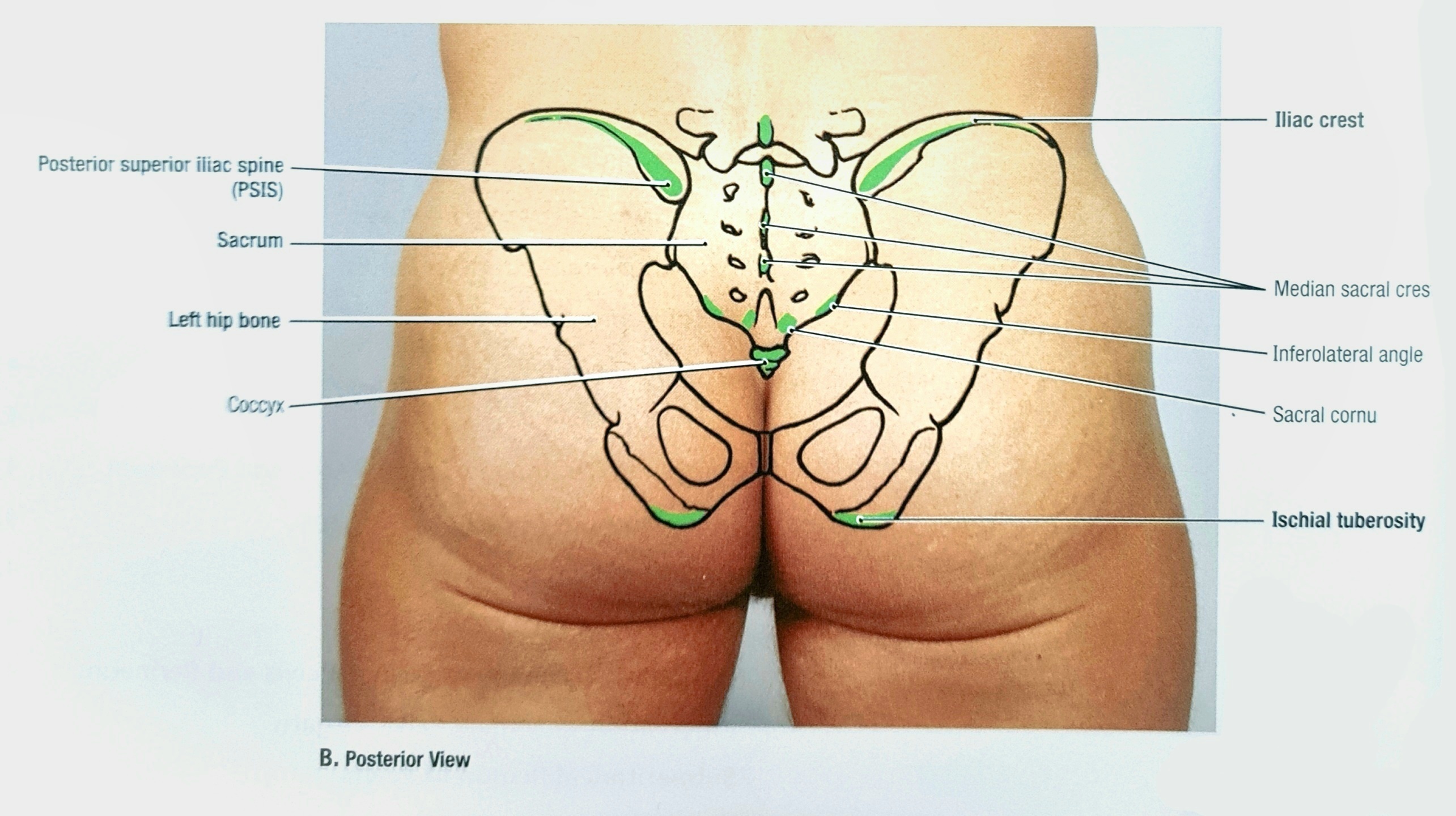
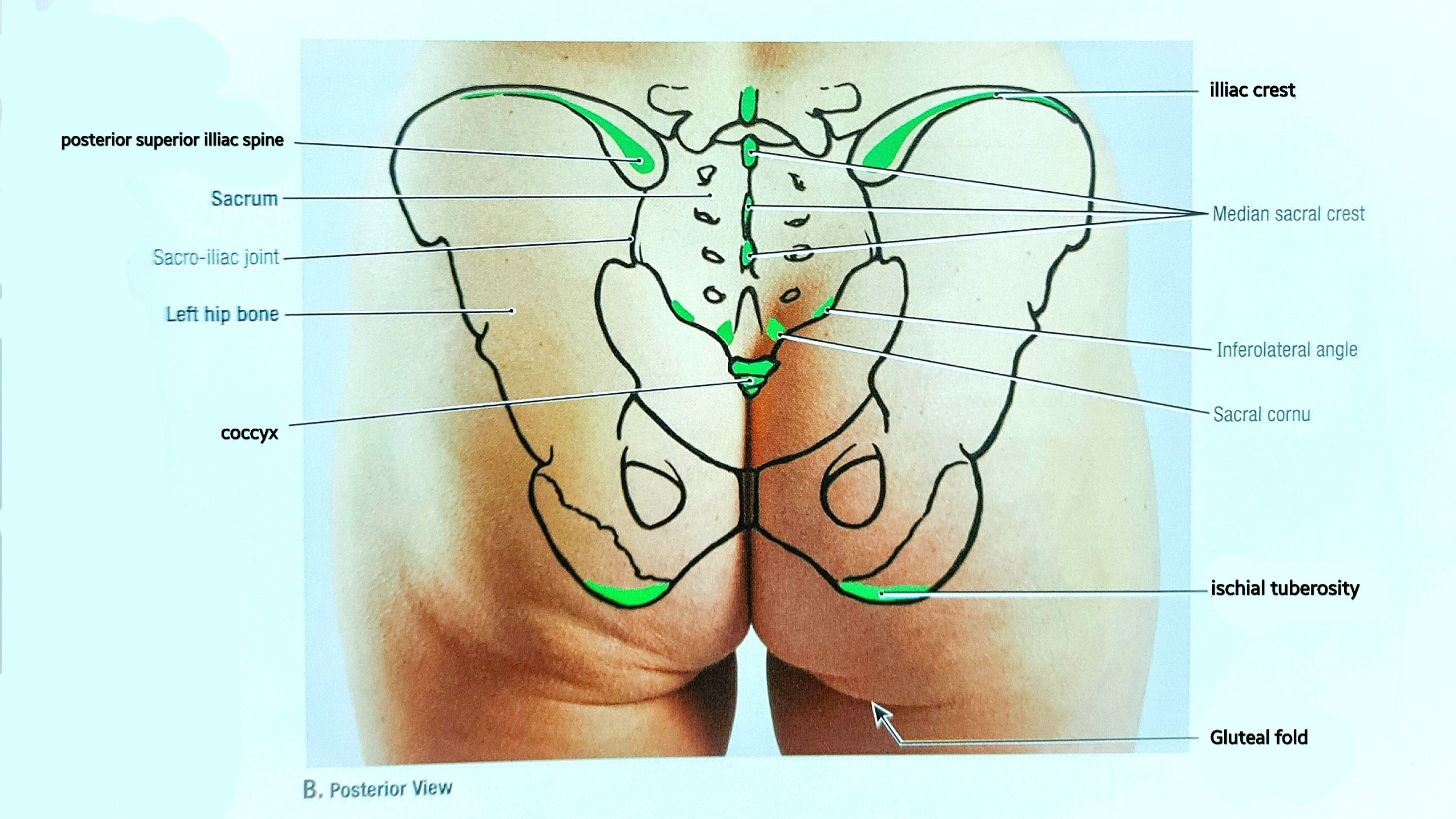
• Palpable structures
Coccyx : you can palpable the coccyx or the tail bone which is the last part of the continuation of the vertebrae column at the proximal end of the Intergluteal cleft, 5 centimeters above and posterior to the anus. It is deeper when the hip is extended.
Greater trochanter : to palpate the greater trochanter have the leg flexed at the knee joint, and the hip abducted to relax the abductor muscles covering it, start to palpate on the lateral side of the buttock until you find the rounded bony structure, rotate the leg medially and lateral to make sure that you reached it.
Ischial tuberosity : to palpate the Ischial tuberosity have the hip or the knee flexed and the patient lying in the prone position, start to palpate using the thumb or the ankle of your hand and palpate below the Gluteal fold until you reach the most prominent bony structure in that spot. This structure bears the body weight while sitting.
Iliac crest : it is the highest point of the buttocks and the highest point of it is at the level of the fourth lumbar spine, which can be palpated at the end of the back trunk.
Posterior superior iliac spine (PSIS) : is palpated at the level of the second sacral spine superior to the coccyx and a bit lateral to the midline.
Greater trochanter : to palpate the greater trochanter have the leg flexed at the knee joint, and the hip abducted to relax the abductor muscles covering it, start to palpate on the lateral side of the buttock until you find the rounded bony structure, rotate the leg medially and lateral to make sure that you reached it.
Ischial tuberosity : to palpate the Ischial tuberosity have the hip or the knee flexed and the patient lying in the prone position, start to palpate using the thumb or the ankle of your hand and palpate below the Gluteal fold until you reach the most prominent bony structure in that spot. This structure bears the body weight while sitting.
Iliac crest : it is the highest point of the buttocks and the highest point of it is at the level of the fourth lumbar spine, which can be palpated at the end of the back trunk.
Posterior superior iliac spine (PSIS) : is palpated at the level of the second sacral spine superior to the coccyx and a bit lateral to the midline.
Gluteal region of Male
Gluteal region of female
• Sensation
To study the sensory innervation of the gluteal region easily we will divide the buttock into four quadrants, and as we know it is symmetrical to the other buttock:
The upper lateral quadrant receives innervation by the lateral branches of the anterior rami of the iliohypogastric (which is originate from the first lumbar spinal nerve) as well as the last (12th) thoracic nerves.
The upper medial quadrant receives innervation from the posterior rami of the upper three lumbar nerves and the upper three sacral nerves.
The lower medial quadrant receives innervation from branches from the posterior cutaneous nerve of the thigh, which originates from the anterior rami of the first three sacral spinal nerves.
The lower lateral quadrant receives innervation from branches of the lateral cutaneous nerve of the thigh, which originates from the anterior rami of the second and third lumbar spinal nerves.
There are some small branches from the last sacral and coccygeal spinal nerves that give sensation to the skin over the coccyx and the floor of the Intergluteal cleft between the two buttocks.
The upper lateral quadrant receives innervation by the lateral branches of the anterior rami of the iliohypogastric (which is originate from the first lumbar spinal nerve) as well as the last (12th) thoracic nerves.
The upper medial quadrant receives innervation from the posterior rami of the upper three lumbar nerves and the upper three sacral nerves.
The lower medial quadrant receives innervation from branches from the posterior cutaneous nerve of the thigh, which originates from the anterior rami of the first three sacral spinal nerves.
The lower lateral quadrant receives innervation from branches of the lateral cutaneous nerve of the thigh, which originates from the anterior rami of the second and third lumbar spinal nerves.
There are some small branches from the last sacral and coccygeal spinal nerves that give sensation to the skin over the coccyx and the floor of the Intergluteal cleft between the two buttocks.
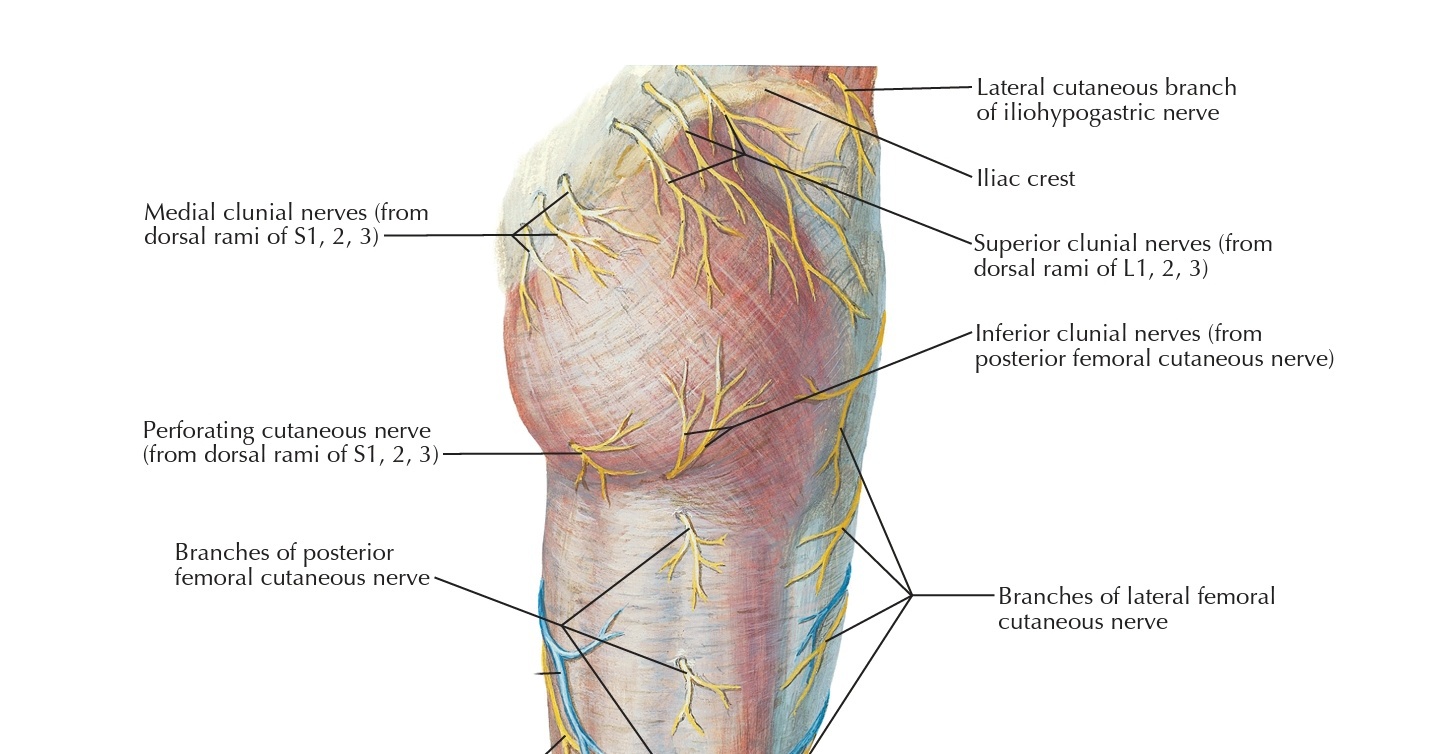
(sensory innervation of the gluteal region)
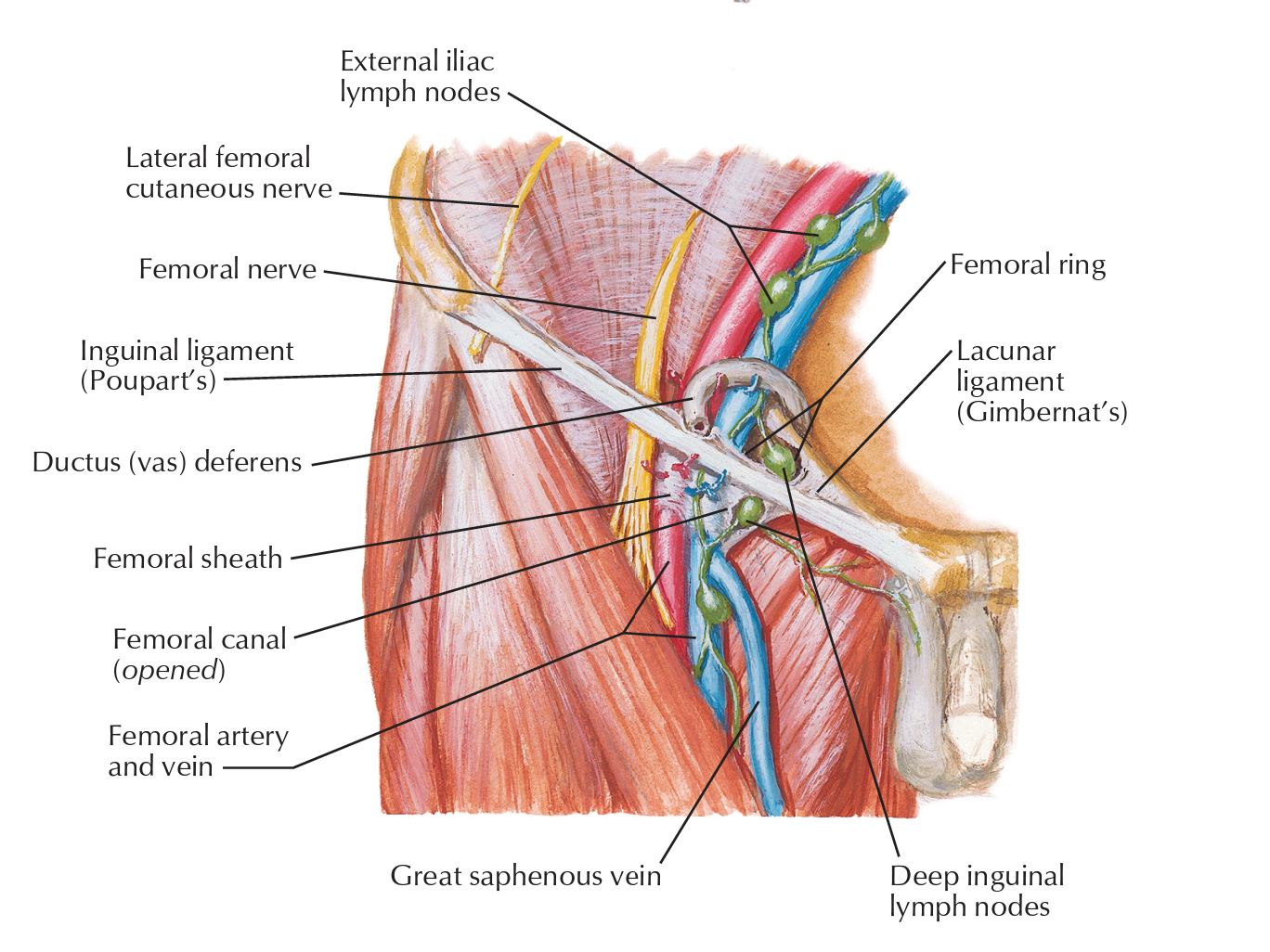
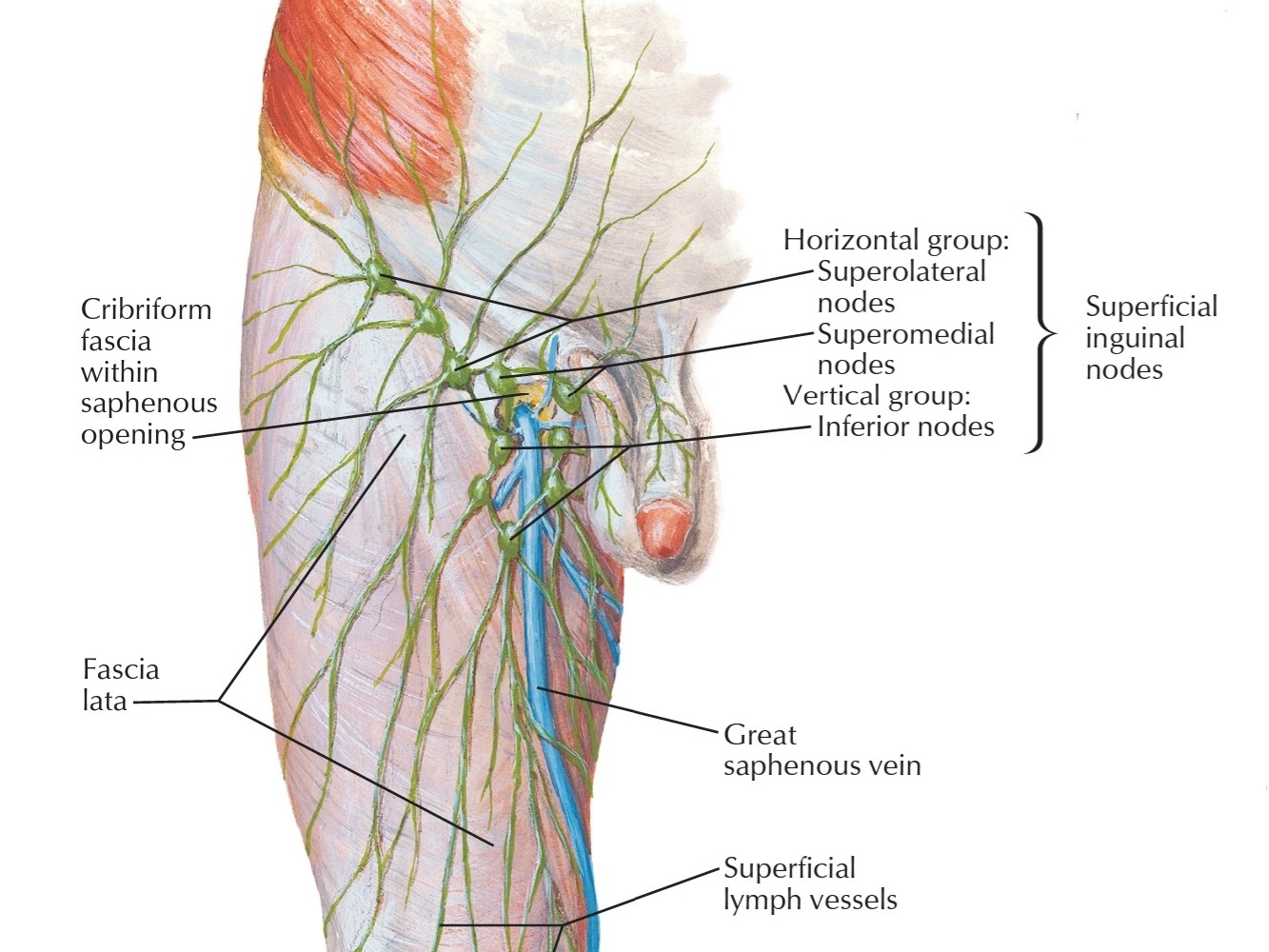
• Lymph
The lymph vessels of the gluteal region drain into the lateral group of the superficial inguinal lymph nodes present below the inguinal ligament and divide into several groups: the superolateral, inferior, and superomedial nodes.
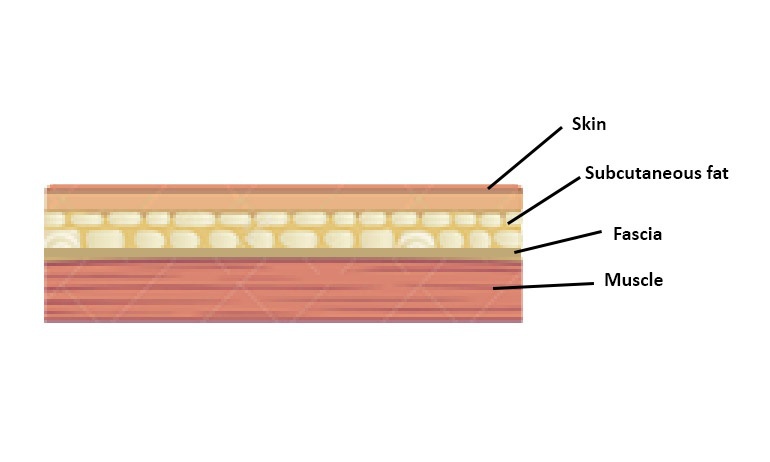
• The fascia
As we know there are two types of fascia, superficial and deep. The superficial fascia in the glutes is thicker that everywhere else in the body, especially in females. It is impregnated with big amounts of fat which give the buttocks their prominences
The deep fascia is continuous below the fascia lata, which covers the thigh like a sleeve. In the gluteal region, the deep fascia splits (divide) into two parts to cover the whole gluteus maximus muscle then continues superiorly, it continues as a single layer that covers the outer surface of the gluteus medius and attaches to the iliac crest of the pelvis.
On the lateral surface of the thigh, there the fascia lata is thickened to form a wide, strong band, the iliotibial tract. This is attached above to the tubercle of the iliac crest and continues inferiorly to the lateral condyle of the tibia bone. The iliotibial tract forms a sheath for the tensor fasciae latae muscle and receives the greater part of the insertion of the gluteus maximus.
The deep fascia is continuous below the fascia lata, which covers the thigh like a sleeve. In the gluteal region, the deep fascia splits (divide) into two parts to cover the whole gluteus maximus muscle then continues superiorly, it continues as a single layer that covers the outer surface of the gluteus medius and attaches to the iliac crest of the pelvis.
On the lateral surface of the thigh, there the fascia lata is thickened to form a wide, strong band, the iliotibial tract. This is attached above to the tubercle of the iliac crest and continues inferiorly to the lateral condyle of the tibia bone. The iliotibial tract forms a sheath for the tensor fasciae latae muscle and receives the greater part of the insertion of the gluteus maximus.
• Nerves and vessels in the gluteal region
The gluteal region communicates with the pelvis cavity through the greater sciatic foramen and with the perineum through the lesser sciatic foramen, important nerves and vessels pass through these foramina to continue their way to other targeted regions in the body.
1. Sciatic Nerve : it enters the lower externalities after originating from the lumbar plexus from the anterior side of the pelvis emerging posteriorly through the greater sciatic foramen, it has a great path in the gluteal region makes it able to get damaged. It then continues its way to reach other parts of the thigh and leg.
2. Superior Gluteal Nerve : it leaves the pelvis after originating from the lumbar plexus, through the upper part of the greater sciatic foramen passing above the piriformis muscle there. Then it continues to reach the muscles that innervate in the gluteal region.
3. Inferior Gluteal Nerve & Nerve to Quadratus Femoris : they leave the pelvis after originating from the lumbar plexus, then passing through the lower part of the greater sciatic foramen posteriorly, finally they reach the muscles which they innervate separately muscle in the gluteal region.
4. Pudendal Nerve and Nerve to Obturator Internus : these nerves leave the pelvis from the greater sciatic foramen and reenter back to the pelvis through the lesser sciatic foramen. They then lie in the posterior aspect of the ischioanal fossa. The pudendal and the nerve to the obturator internus arrive at their last muscle on its pelvic surface and end there.
* There are also some important arteries in the gluteal region such as the superior and inferior gluteal arteries both originating from the internal iliac artery , and give important blood supply in these areas.
1. Sciatic Nerve : it enters the lower externalities after originating from the lumbar plexus from the anterior side of the pelvis emerging posteriorly through the greater sciatic foramen, it has a great path in the gluteal region makes it able to get damaged. It then continues its way to reach other parts of the thigh and leg.
2. Superior Gluteal Nerve : it leaves the pelvis after originating from the lumbar plexus, through the upper part of the greater sciatic foramen passing above the piriformis muscle there. Then it continues to reach the muscles that innervate in the gluteal region.
3. Inferior Gluteal Nerve & Nerve to Quadratus Femoris : they leave the pelvis after originating from the lumbar plexus, then passing through the lower part of the greater sciatic foramen posteriorly, finally they reach the muscles which they innervate separately muscle in the gluteal region.
4. Pudendal Nerve and Nerve to Obturator Internus : these nerves leave the pelvis from the greater sciatic foramen and reenter back to the pelvis through the lesser sciatic foramen. They then lie in the posterior aspect of the ischioanal fossa. The pudendal and the nerve to the obturator internus arrive at their last muscle on its pelvic surface and end there.
* There are also some important arteries in the gluteal region such as the superior and inferior gluteal arteries both originating from the internal iliac artery , and give important blood supply in these areas.
REFERENCES
• Snell's clinical anatomy by Region's (10th edition) pages 1268-1287
• Adam W. M. Mitchell, A. Wayne Vogl, Richard L. Drake, Gray's Anatomy for students (4th edition) page 566,659
• Anatomy, Abdomen and Pelvis, Inguinal Lymph Node Bui T, Bordoni B. 2022, jan. National library of medicine https://www.ncbi.nlm.nih.gov/books/NBK557639/#:~:text=The%20superficial%20inguinal%20lymph%20nodes,extremity%2C%20scrotum%2C%20and%20vulva.
• Adam W. M. Mitchell, A. Wayne Vogl, Richard L. Drake, Gray's Anatomy for students (4th edition) page 566,659
• Anatomy, Abdomen and Pelvis, Inguinal Lymph Node Bui T, Bordoni B. 2022, jan. National library of medicine https://www.ncbi.nlm.nih.gov/books/NBK557639/#:~:text=The%20superficial%20inguinal%20lymph%20nodes,extremity%2C%20scrotum%2C%20and%20vulva.
IMAGES REFERENCES
• Cover image by Gluteal region and leg, illustration by https://www.sciencephoto.com/media/1076514/view/gluteal-region-and-leg-illustration
• Fig1 fig6 & 7 Frank H. Netter, Atlas of Human Anatomy (7th edition) plate 152, 471-472
• Fig2 & fig3 Anne M. R. Agur & Arthur F. Dalley Grant's Atlas of Anatomy 15th edition pages 392-393
• Fig4 Snell's clinical anatomy by Region's (10th edition) Figure 1.12 Cutaneous nerves of the posterior surface of the right lower limb
• Fig8 Simplified representation of skin and fascia layers Figure 1 academy of clinical massage https://www.academyofclinicalmassage.com/elongate_fascia_pt2/
• Fig1 fig6 & 7 Frank H. Netter, Atlas of Human Anatomy (7th edition) plate 152, 471-472
• Fig2 & fig3 Anne M. R. Agur & Arthur F. Dalley Grant's Atlas of Anatomy 15th edition pages 392-393
• Fig4 Snell's clinical anatomy by Region's (10th edition) Figure 1.12 Cutaneous nerves of the posterior surface of the right lower limb
• Fig8 Simplified representation of skin and fascia layers Figure 1 academy of clinical massage https://www.academyofclinicalmassage.com/elongate_fascia_pt2/