Radius
By : Sara OthmanOverview
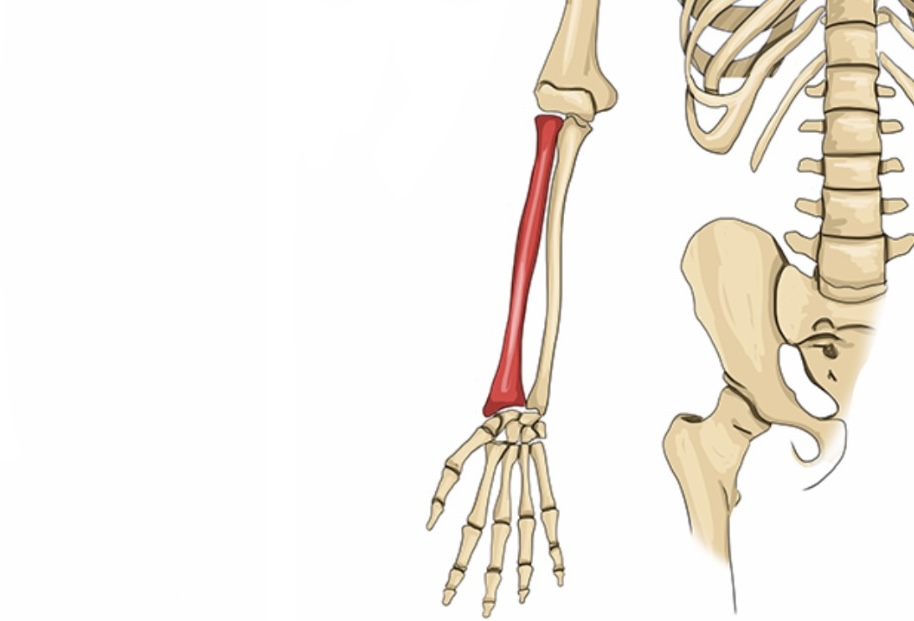
The radius is smaller and shorter than ulna.
Type:- long bone
Location:- on the lateral side of the forearm and parallel to the ulna .
Its head on the proximal end .
During supination and pronation is rotates around ulna.
Type:- long bone
Location:- on the lateral side of the forearm and parallel to the ulna .
Its head on the proximal end .
During supination and pronation is rotates around ulna.
Bony parts
A) Proximally
1- The head is rounded and has two articular surfaces:
1.Superiorly it has a smooth concave surface to articulate with the capitulum of humerus at elbow joined
2.Medially the articular surface articulate with the radial notch of the ulna to form the proximal radioulnar joint.
2- The neck is located distal to the head.
3- The radial tuberosity is oval prominent on the anteromedial surface, distal to the neck, it separates the proximal end ( head & neck ) from the shaft.
*the biceps brachii m. makes insertion on it.
4- The shaft is narrow above and enlarged below , it has three borders there :
1.Anterior border
2.Posterior border
3.Medial border which has a sharp crest ( interosseous border ) for the attachment of interosseous membrane ( between ulna & radius ).
And has three surfaces there :
1.Anterior surface
2.Posterior surface
3.Lateral surface
B) Distally
From the distal surface there is a carpal articular surface which articulates to form wrist joint.
5- The ulnar notch on the medial aspect of the distal forth of radius is a smooth , shallow depression which articulates with head of ulna to form the distal radioulnar joint.
6- The styloid process is a small , conical projection from the lateral , distal aspect of the bone , is larger than the ulnar styloid process ( this has a clinical importance in the identifying of the fractured bone ) , it forms the insertion site of brachioradialis m.
7- The dorsal tubercle is a projection that is located posteriorly on the distal end of the radius between two grooves that transmit the tendons of forearm muscles , it can be palpated on the dorsum of hand.
1- The head is rounded and has two articular surfaces:
1.Superiorly it has a smooth concave surface to articulate with the capitulum of humerus at elbow joined
2.Medially the articular surface articulate with the radial notch of the ulna to form the proximal radioulnar joint.
2- The neck is located distal to the head.
3- The radial tuberosity is oval prominent on the anteromedial surface, distal to the neck, it separates the proximal end ( head & neck ) from the shaft.
*the biceps brachii m. makes insertion on it.
4- The shaft is narrow above and enlarged below , it has three borders there :
1.Anterior border
2.Posterior border
3.Medial border which has a sharp crest ( interosseous border ) for the attachment of interosseous membrane ( between ulna & radius ).
And has three surfaces there :
1.Anterior surface
2.Posterior surface
3.Lateral surface
B) Distally
From the distal surface there is a carpal articular surface which articulates to form wrist joint.
5- The ulnar notch on the medial aspect of the distal forth of radius is a smooth , shallow depression which articulates with head of ulna to form the distal radioulnar joint.
6- The styloid process is a small , conical projection from the lateral , distal aspect of the bone , is larger than the ulnar styloid process ( this has a clinical importance in the identifying of the fractured bone ) , it forms the insertion site of brachioradialis m.
7- The dorsal tubercle is a projection that is located posteriorly on the distal end of the radius between two grooves that transmit the tendons of forearm muscles , it can be palpated on the dorsum of hand.
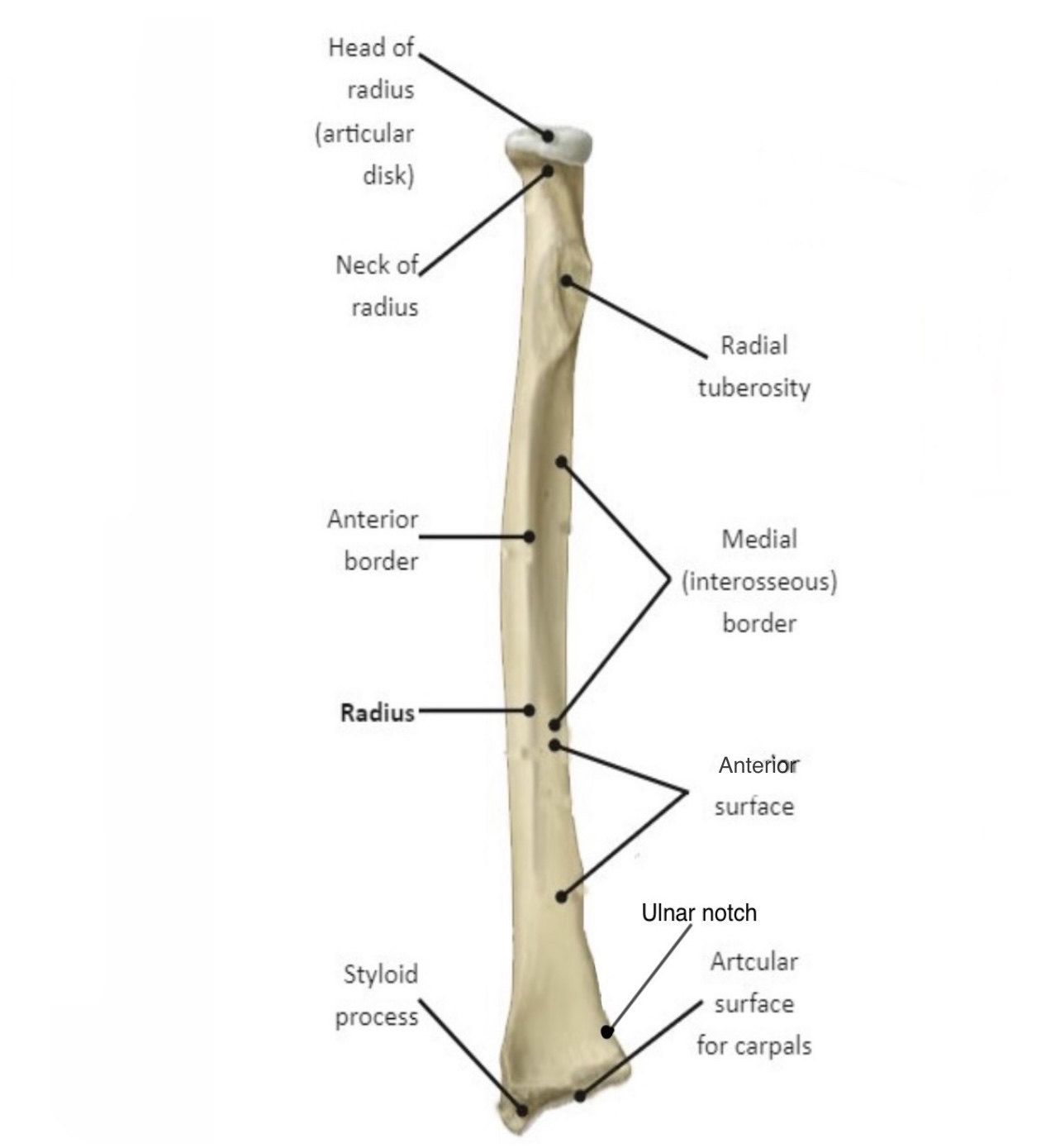
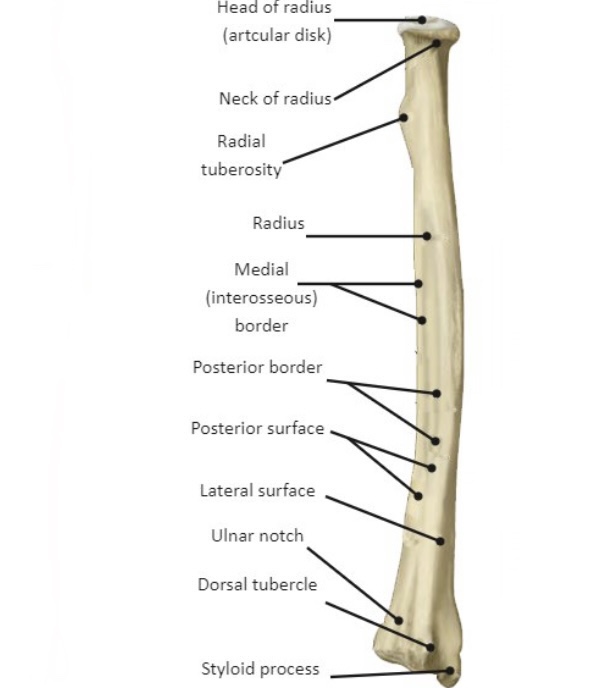
Anterior view of right radius
How to know the bone is right or left
1- The head should be superiorly directed.
2- The radial tuberosity should be on the anteromedial surface of the bone.
3- The styloid process should be laterally directed.
2- The radial tuberosity should be on the anteromedial surface of the bone.
3- The styloid process should be laterally directed.
The articulation
The radius has four places to form four joint:-
1- It shares with elbow joint where it articulates with capitulum through the superior surface of its head.
2- The proximal radioulnar joint between the medial surface of the head of radius and the radial notch of ulna.
3- The distal radioulnar joint between the ulnar notch of radius and the head of ulna.
4- The carpal articular surface of the radius articulates medially with lunate bone and laterally with scaphoid bone to form wrist joint.
1- It shares with elbow joint where it articulates with capitulum through the superior surface of its head.
2- The proximal radioulnar joint between the medial surface of the head of radius and the radial notch of ulna.
3- The distal radioulnar joint between the ulnar notch of radius and the head of ulna.
4- The carpal articular surface of the radius articulates medially with lunate bone and laterally with scaphoid bone to form wrist joint.
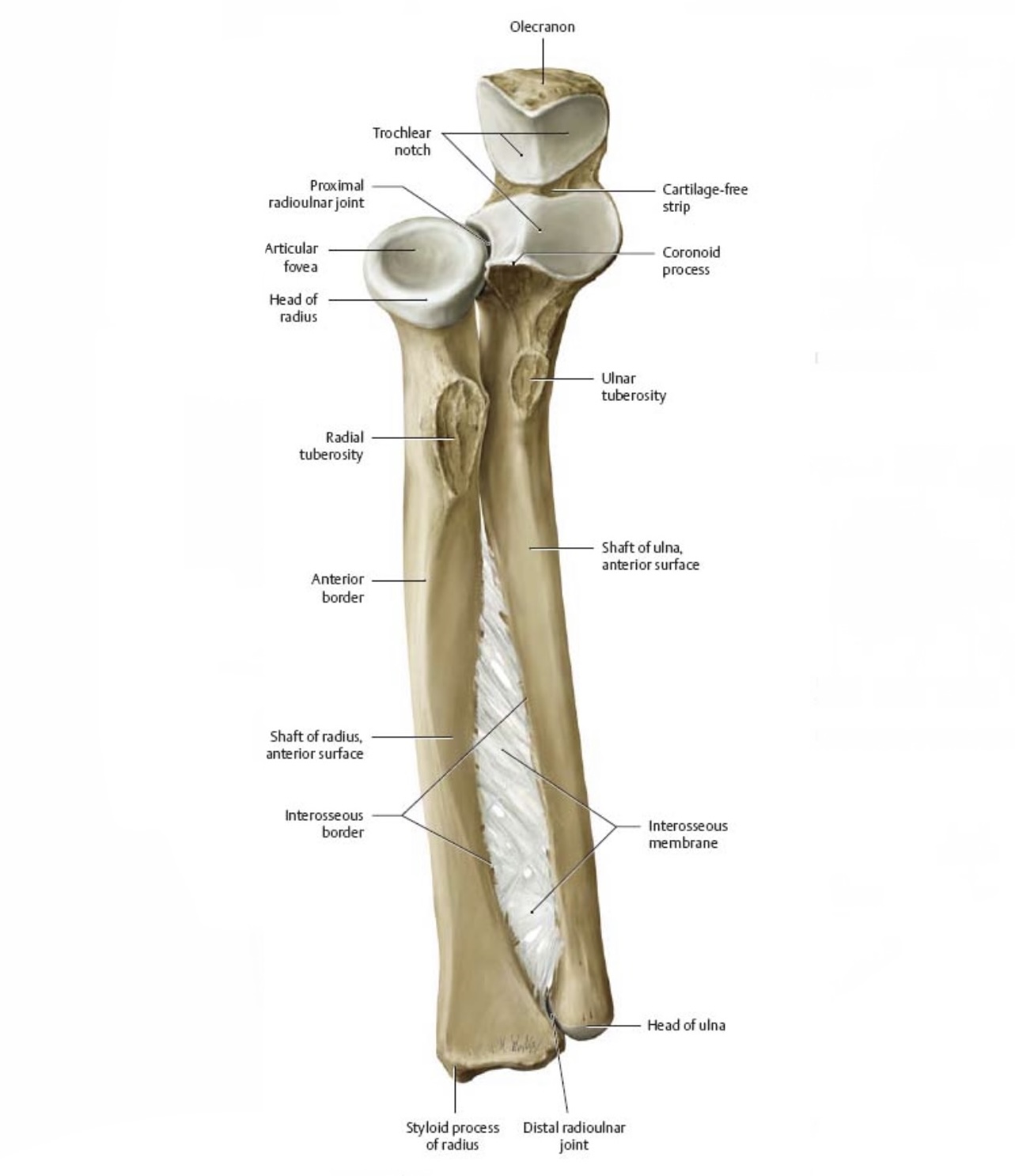
proximal & distal radioulnar joint
Muscles attached to the bone
The shaft of radius gives origin to four muscles :-
1- radial head of flexor digitorum superficialis & flexor pollicis longus on anterior surface of the bone.
2- abductor pollicis longus & extensor pollicis brevis on posterior surface of the bone.
And receive the insertion of five muscles :-
1- biceps brachii at radial tuberosity.
2- supinator & pronater teres at lateral aspect of the bone.
3- pronator quadratus at distal fourth of anterior surface.
4- brachioradialis at lateral side of distal end.
1- radial head of flexor digitorum superficialis & flexor pollicis longus on anterior surface of the bone.
2- abductor pollicis longus & extensor pollicis brevis on posterior surface of the bone.
And receive the insertion of five muscles :-
1- biceps brachii at radial tuberosity.
2- supinator & pronater teres at lateral aspect of the bone.
3- pronator quadratus at distal fourth of anterior surface.
4- brachioradialis at lateral side of distal end.
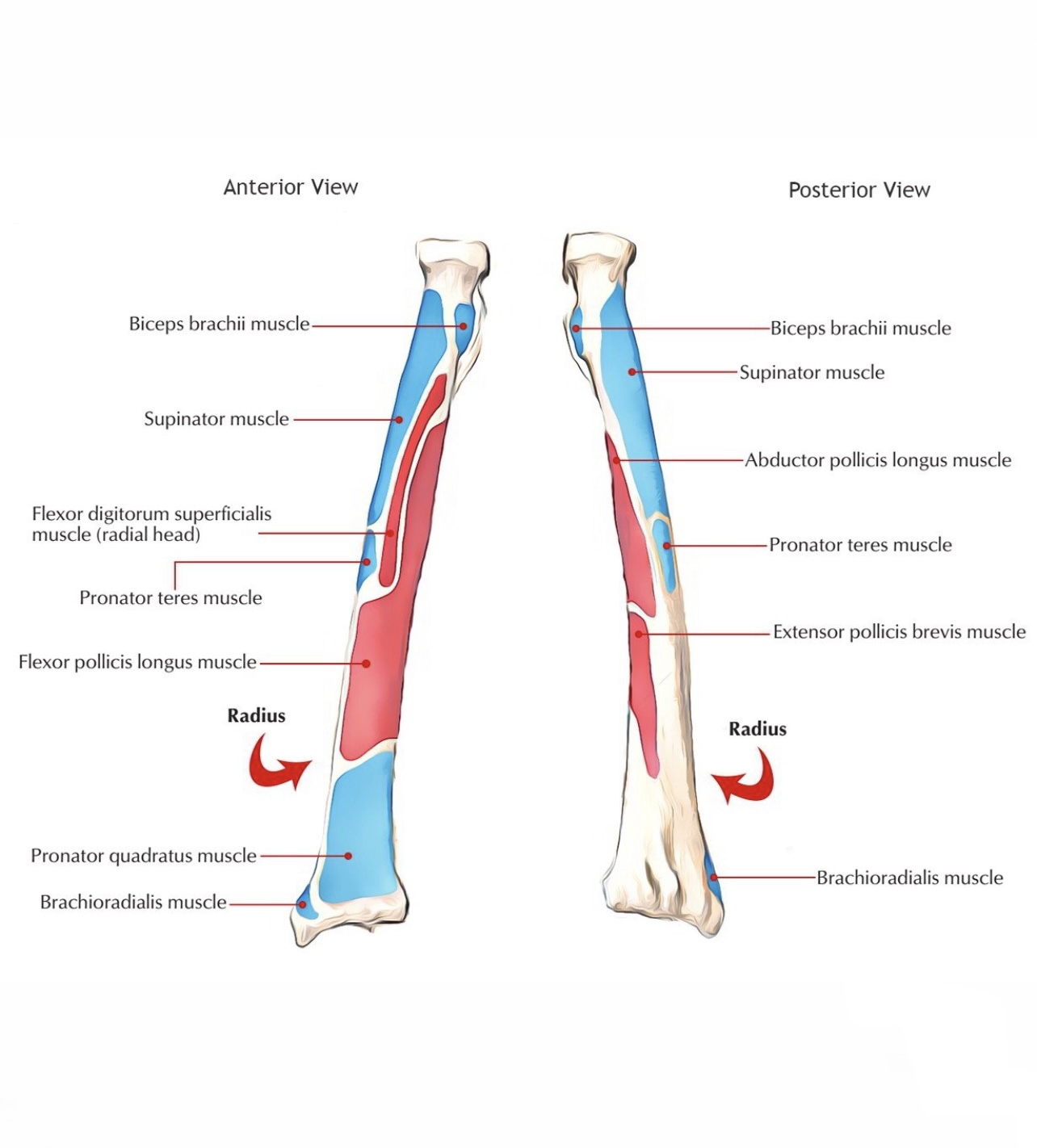
Attachments of radius
The fractures
The fracture of radius may be associated with the fracture or dislocation of ulna because they are connected by strong interosseous membrane.
*the fracture of the distal end of radius may hurts the radial a. which winds posteriorly at the distal end of the radius.
*the pulsation of the radial a. can be palpated against the distal end of the radius close to the lateral side of flexor carpi radialis tendon .
Monteggia fracture :- is the fracture of ulna and dislocation of the head of radius ( the proximal radioulnar joint ).
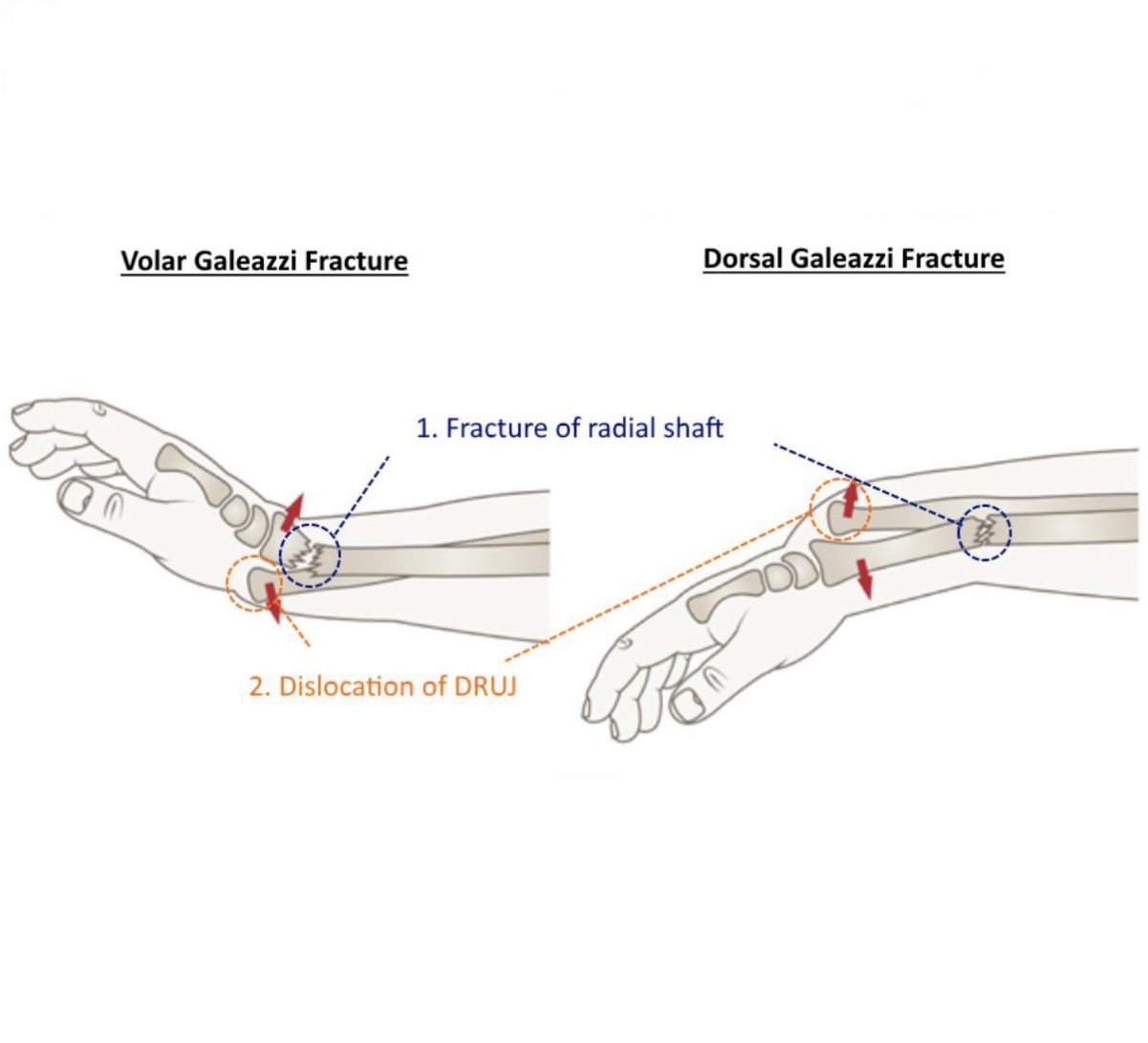
Galeazzi fracture:- is the isolated fracture of the junction between the middle and distal third of radius accompanied by the dislocation of the distal radioulnar joint ( dorsal or volar dislocation ),it limited forearm rang of motion, it could be occurred due the direct wrist trauma and falling onto outstretched hand with a pronated forearm.
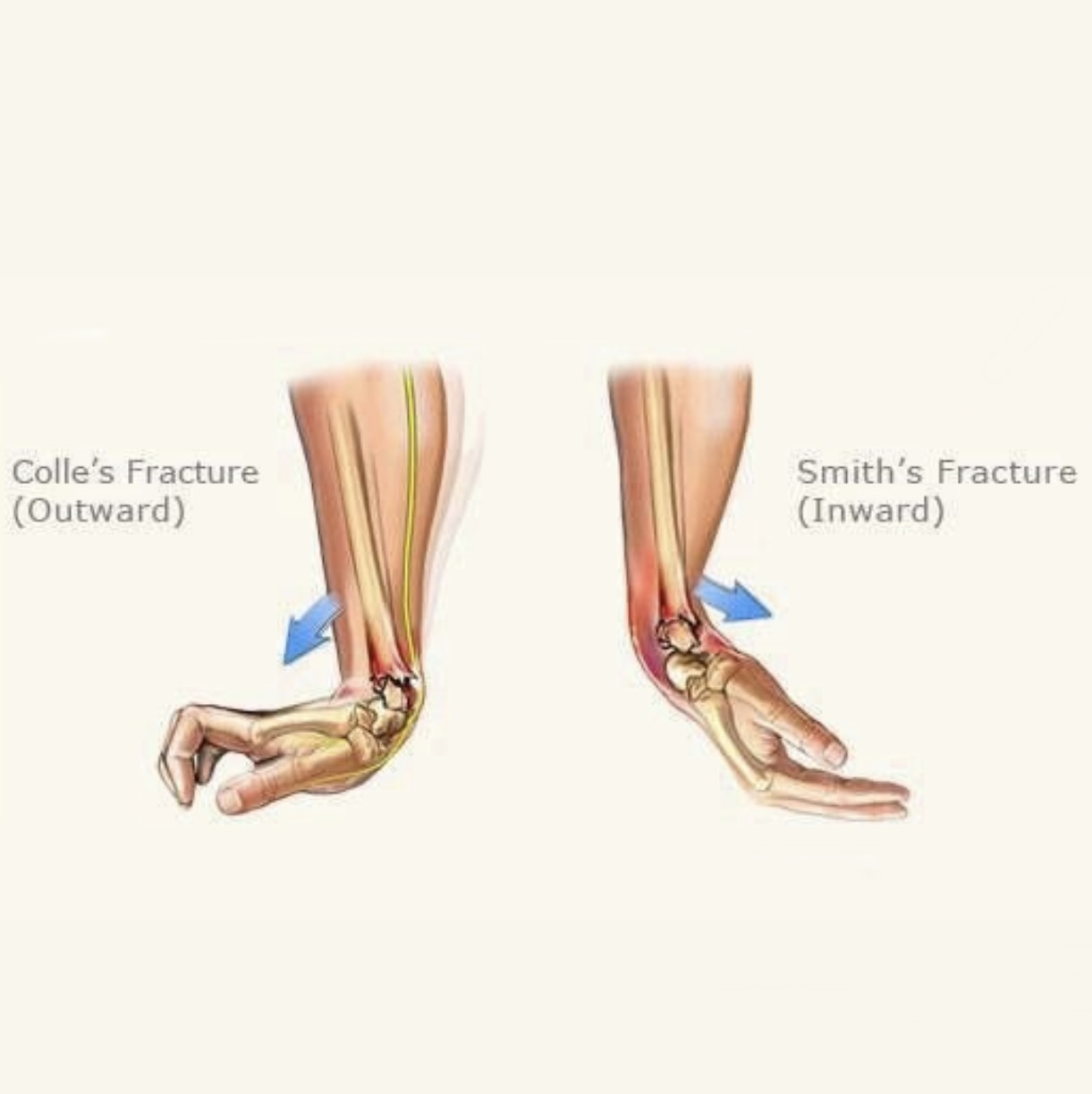
Colle’s fracture :- is the most common fracture of the distal end of radius. It is a very painful and serious injury that commonly occurs with osteoporosis patient and people older than 50 years after a fall on an outstretched hand or a trauma like car crash , skiing , bike riding or other accident.
The bone fractures transversally and the distal end inclines posteriorly and the posterior dislocation of the articular surface make the point looks like fork from the side and that’s called ( dinner-fork deformity ) and that can lead to malunion ( where the bones fail to fuse ).
The other complications that could be occurred are:
1.Carpal tunnel syndrome ( compression of median n. )
2.Compartment syndrome ( muscle pressure reaching dangerous levels )
3.Reflex sympathetic dystrophy causes burning pain in your arms, legs, hands or feet
4.Secondary osteoarthritis in the wrist ( pain and swelling )
5. EPL ( the extensor pollicis longus ) tendon tear ( loss extension of the end joint of the thumb and weak extension of the thumb ).
* the extension is straightening the joint.
Smith’s fracture :- it is also happened in the distal end of the radius from a direct blow or a fall on the dorsum of the flexed hand , car accidents or other traumas. It is the reversed of colles fracture, where the broken end of the bone is directed anteriorly. It occurs to people older than 50 years , and is more common in women than men.
The complications of this fracture are:
1.Acute compartment syndrome (ACS): A build-up of pressure in the muscles may inhibit blood from getting to tissue
2.Malunion ( where the bones fail to fuse )
3.Carpal tunnel syndrome ( compression of median n. )
4.Bone infection (osteomyelitis) is an open wrist fracture. It increase the risk of bacterial infection and other internal damage ( damage muscles, nerves, blood vessels, tendons and ligaments around the injury ).
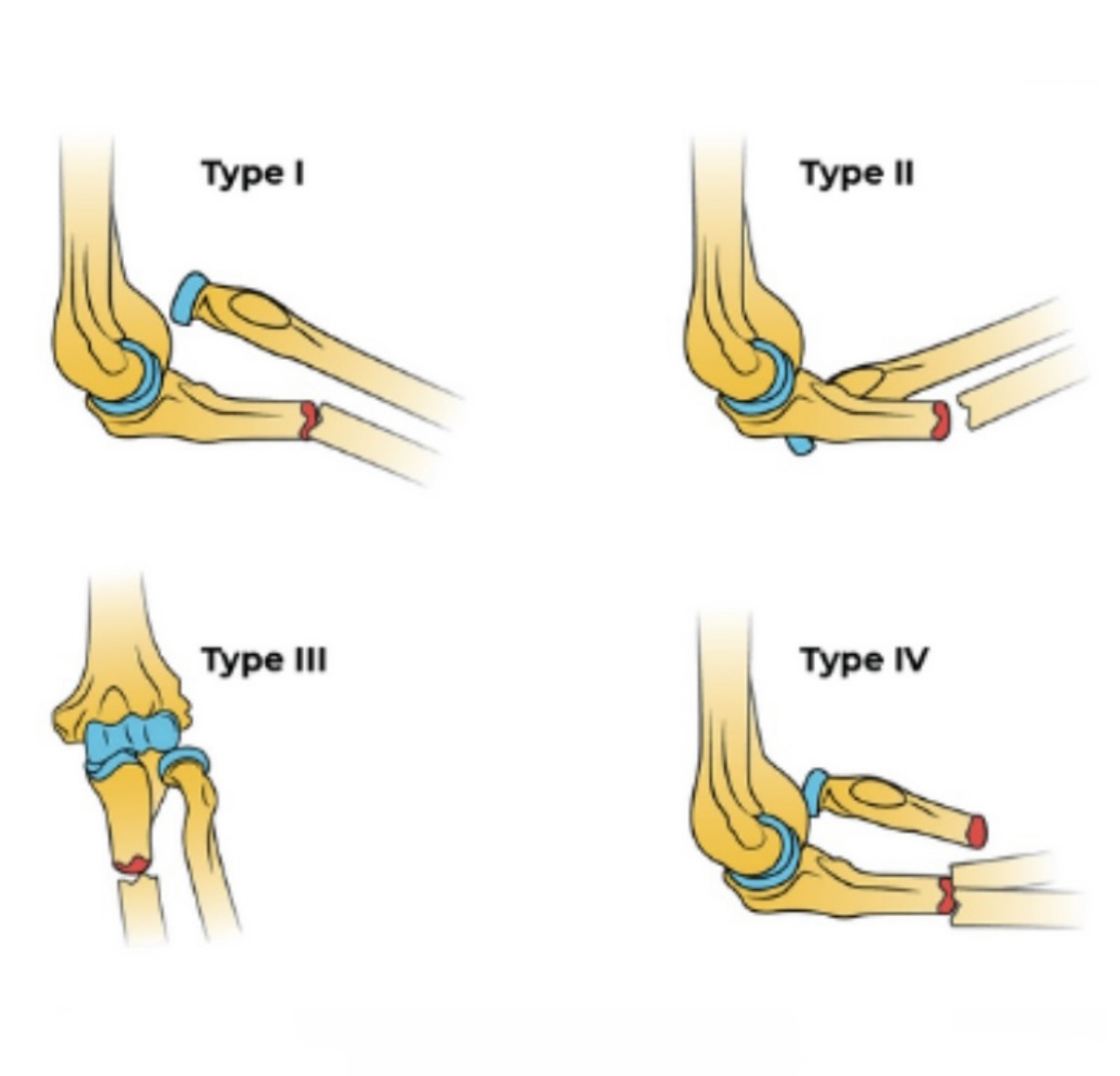
Smith fracture is divided into three type :-
A) type l :- about 85% of cases , is an extra-articular fracture through the distal radius.
B) type ll :- about 13%, is an intra-articular oblique fracture.
C) type lll :- less than 2%, is a juxta-articular oblique fracture.
*the fracture of the distal end of radius may hurts the radial a. which winds posteriorly at the distal end of the radius.
*the pulsation of the radial a. can be palpated against the distal end of the radius close to the lateral side of flexor carpi radialis tendon .
Monteggia fracture :- is the fracture of ulna and dislocation of the head of radius ( the proximal radioulnar joint ).
Galeazzi fracture:- is the isolated fracture of the junction between the middle and distal third of radius accompanied by the dislocation of the distal radioulnar joint ( dorsal or volar dislocation ),it limited forearm rang of motion, it could be occurred due the direct wrist trauma and falling onto outstretched hand with a pronated forearm.
Colle’s fracture :- is the most common fracture of the distal end of radius. It is a very painful and serious injury that commonly occurs with osteoporosis patient and people older than 50 years after a fall on an outstretched hand or a trauma like car crash , skiing , bike riding or other accident.
The bone fractures transversally and the distal end inclines posteriorly and the posterior dislocation of the articular surface make the point looks like fork from the side and that’s called ( dinner-fork deformity ) and that can lead to malunion ( where the bones fail to fuse ).
The other complications that could be occurred are:
1.Carpal tunnel syndrome ( compression of median n. )
2.Compartment syndrome ( muscle pressure reaching dangerous levels )
3.Reflex sympathetic dystrophy causes burning pain in your arms, legs, hands or feet
4.Secondary osteoarthritis in the wrist ( pain and swelling )
5. EPL ( the extensor pollicis longus ) tendon tear ( loss extension of the end joint of the thumb and weak extension of the thumb ).
* the extension is straightening the joint.
Smith’s fracture :- it is also happened in the distal end of the radius from a direct blow or a fall on the dorsum of the flexed hand , car accidents or other traumas. It is the reversed of colles fracture, where the broken end of the bone is directed anteriorly. It occurs to people older than 50 years , and is more common in women than men.
The complications of this fracture are:
1.Acute compartment syndrome (ACS): A build-up of pressure in the muscles may inhibit blood from getting to tissue
2.Malunion ( where the bones fail to fuse )
3.Carpal tunnel syndrome ( compression of median n. )
4.Bone infection (osteomyelitis) is an open wrist fracture. It increase the risk of bacterial infection and other internal damage ( damage muscles, nerves, blood vessels, tendons and ligaments around the injury ).
Smith fracture is divided into three type :-
A) type l :- about 85% of cases , is an extra-articular fracture through the distal radius.
B) type ll :- about 13%, is an intra-articular oblique fracture.
C) type lll :- less than 2%, is a juxta-articular oblique fracture.

Monteggia fracture
References
1- Moore's Clinically Oriented Anatomy 7th Edition / pp.678-679 , pp.685-686
2- LAWRENCE E. WINESKI Snell's Clinical Anatomy by Regions /10th Edition (2018 ) / pp.92 , pp.94-95-96
3- the radius , Author: Oliver Jones , Source: TeachMe Anatomy , https://teachmeanatomy.info/upper-limb/bones/radius/
4- smith’s fracture , Author: Jeremy D. Schroeder, Matthew Varacallo , Source: NCBI Bookshelf , https://www.ncbi.nlm.nih.gov/books/NBK547714/
5- colle’s fracture , Source:Cleveland Clinic , https://my.clevelandclinic.org/health/diseases/21860-colles-fracture
2- LAWRENCE E. WINESKI Snell's Clinical Anatomy by Regions /10th Edition (2018 ) / pp.92 , pp.94-95-96
3- the radius , Author: Oliver Jones , Source: TeachMe Anatomy , https://teachmeanatomy.info/upper-limb/bones/radius/
4- smith’s fracture , Author: Jeremy D. Schroeder, Matthew Varacallo , Source: NCBI Bookshelf , https://www.ncbi.nlm.nih.gov/books/NBK547714/
5- colle’s fracture , Source:Cleveland Clinic , https://my.clevelandclinic.org/health/diseases/21860-colles-fracture
References of images
_Cover image: Source: Mammoth Memory , https://www.google.com/imgres?imgurl=https%3A%2F%2Fmammothmemory.net%2Fimages%2Fuser%2Fbase%2Funcategorised%2F1.32.19%2520Location%2520of%2520the%2520radius.jpg&imgrefurl=https%3A%2F%2Fmammothmemory.net%2Fbiology%2Fskeletons-and-bones%2Fskeleton-and-bones%2Fthe-radius.html&tbnid=RxO_RXRFfsPz0M&vet=1&docid=f7Vy_5SXvhwmwM&w=750&h=500&itg=1&hl=ar&source=sh%2Fx%2Fim
_Figure1&2 : Anterior & posterior view od right radius, Source: EdrawMax, https://images.app.goo.gl/w6Fy6C2QyALE2k7M9
_Figure3 : proximal & distal radioulnar joint , Source: docrtorlib.info , https://images.app.goo.gl/paSjU2WmNEFBsKPc7
_Figure4 : attachments of radius , Source: Eartn’s Lab , https://images.app.goo.gl/ZATvVuDBxEKqib999
_Figure5 : Monteggia fracture , source: Don’t forget the Bubbles , https://images.app.goo.gl/Jm7YmhMN59tjrYRL6
_Figure6 : Galeazzi fracture , source: hotcore.info , https://images.app.goo.gl/4t698srfss4MKcqT6
_Figure7 : dinner like deformity, Source: Mobile Physiotherapy Clinic , https://www.google.com/imgres?imgurl=https%3A%2F%2Fmobilephysiotherapyclinic.in%2Fwp-content%2Fuploads%2F2017%2F08%2FDinner-Fork-Deformity.jpg&imgrefurl=https%3A%2F%2Fmobilephysiotherapyclinic.in%2Fdinner-fork-deformity-exercise%2F&tbnid=-8eqfmMDRRR2rM&vet=1&docid=5noKTPty8cTngM&w=960&h=720&hl=ar&source=sh%2Fx%2Fim
_Figure8 : EPL tendon rupture, Source: Scientific Research Publishing , https://www.google.com/imgres?imgurl=https%3A%2F%2Fhtml.scirp.org%2Ffile%2F2-2010665x3.png&imgrefurl=https%3A%2F%2Fwww.scirp.org%2Fjournal%2Fpaperinformation.aspx%3Fpaperid%3D97358&tbnid=CVe1puYBJm99nM&vet=1&docid=ve3l81dRCmQEKM&w=420&h=314&hl=ar&source=sh%2Fx%2Fim
_Figure9 : Colle’s & Smith’s fractures , Source: Ladisten, https://images.app.goo.gl/DWDDNrAKhH6WswYm6
_Figure1&2 : Anterior & posterior view od right radius, Source: EdrawMax, https://images.app.goo.gl/w6Fy6C2QyALE2k7M9
_Figure3 : proximal & distal radioulnar joint , Source: docrtorlib.info , https://images.app.goo.gl/paSjU2WmNEFBsKPc7
_Figure4 : attachments of radius , Source: Eartn’s Lab , https://images.app.goo.gl/ZATvVuDBxEKqib999
_Figure5 : Monteggia fracture , source: Don’t forget the Bubbles , https://images.app.goo.gl/Jm7YmhMN59tjrYRL6
_Figure6 : Galeazzi fracture , source: hotcore.info , https://images.app.goo.gl/4t698srfss4MKcqT6
_Figure7 : dinner like deformity, Source: Mobile Physiotherapy Clinic , https://www.google.com/imgres?imgurl=https%3A%2F%2Fmobilephysiotherapyclinic.in%2Fwp-content%2Fuploads%2F2017%2F08%2FDinner-Fork-Deformity.jpg&imgrefurl=https%3A%2F%2Fmobilephysiotherapyclinic.in%2Fdinner-fork-deformity-exercise%2F&tbnid=-8eqfmMDRRR2rM&vet=1&docid=5noKTPty8cTngM&w=960&h=720&hl=ar&source=sh%2Fx%2Fim
_Figure8 : EPL tendon rupture, Source: Scientific Research Publishing , https://www.google.com/imgres?imgurl=https%3A%2F%2Fhtml.scirp.org%2Ffile%2F2-2010665x3.png&imgrefurl=https%3A%2F%2Fwww.scirp.org%2Fjournal%2Fpaperinformation.aspx%3Fpaperid%3D97358&tbnid=CVe1puYBJm99nM&vet=1&docid=ve3l81dRCmQEKM&w=420&h=314&hl=ar&source=sh%2Fx%2Fim
_Figure9 : Colle’s & Smith’s fractures , Source: Ladisten, https://images.app.goo.gl/DWDDNrAKhH6WswYm6