Distal Radioulnar Joint Injuries And Instability
By : Yaser MohammedDistal Radioulnar Joint Injuries
Distal radioulnar joint (DRUJ) injuries can occur separately or in conjunction with distal radius fractures and both-bone forearm fractures. In fact, nearly 60 percent of forearm fractures adversely affect the DRUJ.
Note:The action of distal and proximal radioulnar joints which are the supination and pronation of the forearm the ulna is stationary, and is the stable anatomical point of reference for the rotation.
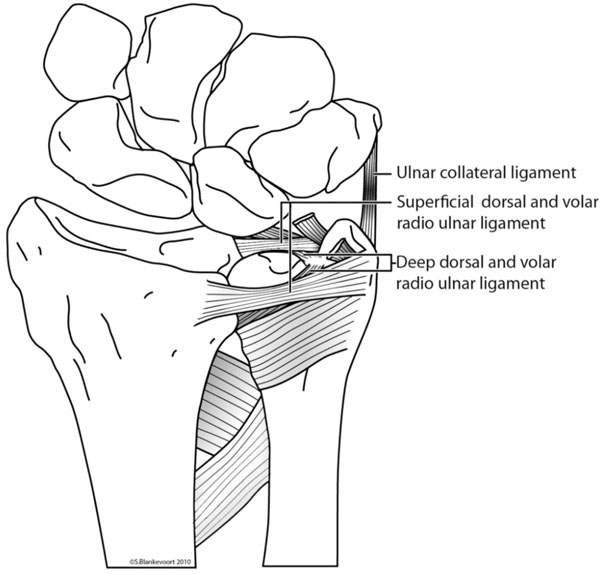
The stability of the DRUJ comes from the fully congruent articulating surfaces and the radioulnar ligaments cover the joint. Following a distal radius fracture, the congruency is lost, and stabilizing ligaments tear.
DRUJ injuries are classified depending on the injured structures and clinical findings as stable, partially unstable (subluxation), and unstable (dislocation) patterns.
Note:The action of distal and proximal radioulnar joints which are the supination and pronation of the forearm the ulna is stationary, and is the stable anatomical point of reference for the rotation.
The stability of the DRUJ comes from the fully congruent articulating surfaces and the radioulnar ligaments cover the joint. Following a distal radius fracture, the congruency is lost, and stabilizing ligaments tear.
DRUJ injuries are classified depending on the injured structures and clinical findings as stable, partially unstable (subluxation), and unstable (dislocation) patterns.

Distal radioulnar joint (DRUJ) injuries
Distal Radioulnar Joint Instability
Distal Radioulnar Joint Instability is a common clinical condition in this joint and is frequently misdiagnosed,
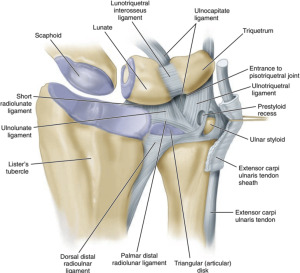
we need to know that the stability of the distal radioulnar joint comes from both the bony structure and the integrity of the surrounding soft tissues including pronator quadratus, the triangular fibrocartilage complex (TFCC) and interosseous membrane.
while The dorsal and palmar radioulnar ligaments are regarded as the major factors of DRUJ stability.
Distal radioulnar joint instability is associated with the following :
• acute distal radioulnar joint dislocation
• distal radial fractures
• triangular fibrocartilage complex injuries
• fracture malunion
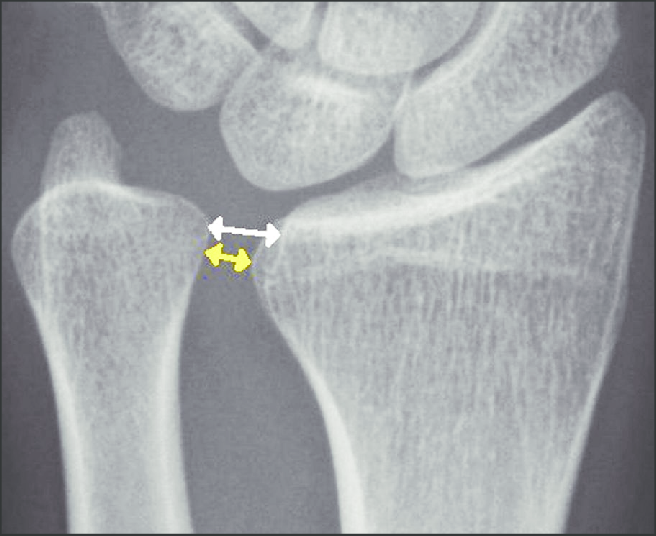
Distal radioulnar joint instability diagnosis is a commonly missed diagnosis that can be easily hidden from clinical and radiographic examinations, Different physical tests for the diagnosis of DRUJ instability have been described, including the Ballottement test (which is considered the most reliable physical examination test for DRUJ instability), radius pull test, clunk test, extensor carpi ulnaris test, and press test.
Both surgical and nonsurgical treatments are possible for DRUJ instability. Nonsurgical treatment can be considered as the primary therapy in less active patients, while surgery used to recover bone and ligament injuries if nonsurgical treatment fails to restore forearm stability and function, surgery is needed.
we need to know that the stability of the distal radioulnar joint comes from both the bony structure and the integrity of the surrounding soft tissues including pronator quadratus, the triangular fibrocartilage complex (TFCC) and interosseous membrane.
while The dorsal and palmar radioulnar ligaments are regarded as the major factors of DRUJ stability.
Distal radioulnar joint instability is associated with the following :
• acute distal radioulnar joint dislocation
• distal radial fractures
• triangular fibrocartilage complex injuries
• fracture malunion
Distal radioulnar joint instability diagnosis is a commonly missed diagnosis that can be easily hidden from clinical and radiographic examinations, Different physical tests for the diagnosis of DRUJ instability have been described, including the Ballottement test (which is considered the most reliable physical examination test for DRUJ instability), radius pull test, clunk test, extensor carpi ulnaris test, and press test.
Both surgical and nonsurgical treatments are possible for DRUJ instability. Nonsurgical treatment can be considered as the primary therapy in less active patients, while surgery used to recover bone and ligament injuries if nonsurgical treatment fails to restore forearm stability and function, surgery is needed.
Distal Radioulnar Joint Instability