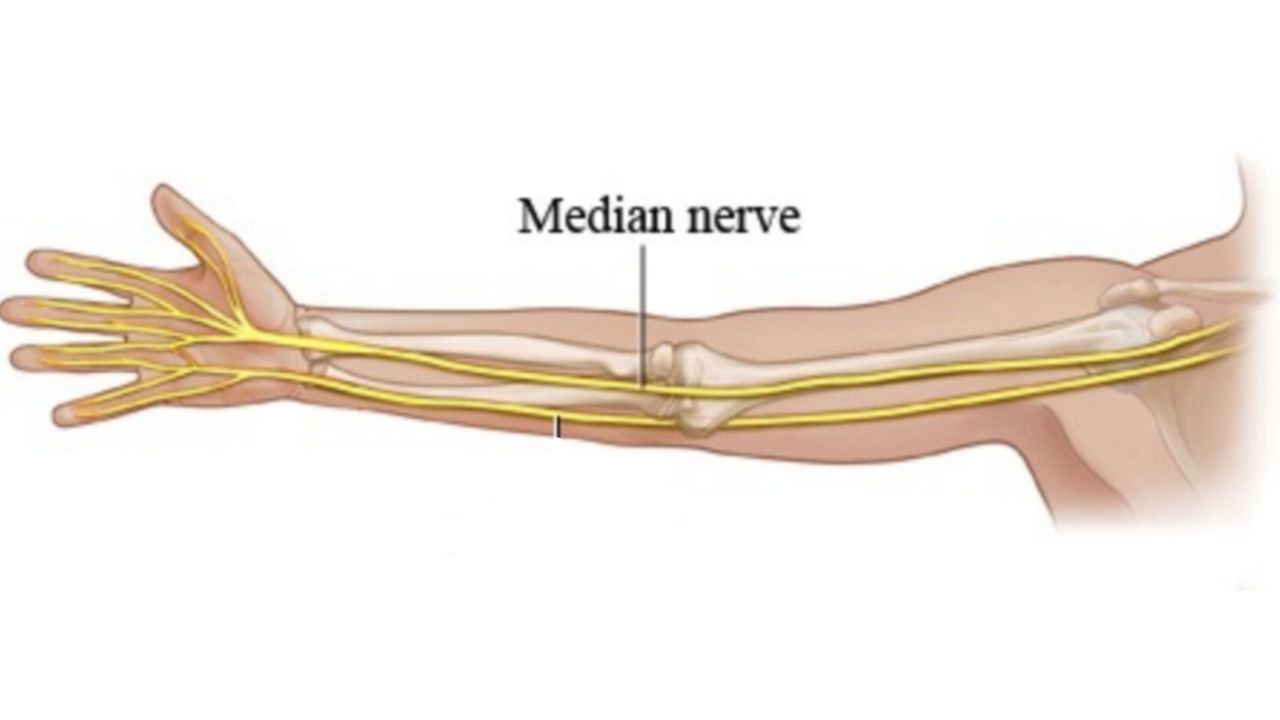
Median nerve
By : Mohammed WaelGeneral
The median nerve is one of the largest branches which supplies the upper limb.
It is originated from:
1. Lateral root ( anterior division of the lateral cord of the brachial plexus)
2. Medial root ( anterior division of the medial cord of the brachial plexus)
The medial and lateral roots unite at the axilla to form the median nerve.
It contains mainly fibers from the anterior rami of spinal nerves C6 , C7 , C8 and T1.
It contains both:
1.Sensory fibers (which gives sensory supply to part of the hand).
2.Motor fibers (which supplies most muscles of the anterior compartment of forearm and hand).
Course And Relation
1. Axilla
It descends lateral to axillary artery then it enters the arm .
2. Arm
As the median nerve reaches the arm , it then runs distally on the lateral side of the brachial artery to the middle of arm where it runs in front of the brachial artery to become medial to the artery below the middle of arm .
It leaves the arm and enters the cubital fossa , in the cubital fossa it lies:
1.Deep to the bicipital aponeurosis and the median cubital vein
2.Medial to the brachial artery
It(the median nerve) has no branches in the arm and cubital fossa except one articulator branch to the elbow joint .
3. Forearm
After the median nerve leaves the cubital fossa , it enters the forearm.
The median nerve is considered as the main nerve of the anterior compartment of the forearm through the anterior interosseous nerve.
It passes between the two heads of the pronator teres muscle.
It descends between flexor digitorum superficialis above & flexor digitorum profundus below.
About 5 cm above wrist, it emerges from lateral border of flexor digitorum superficialis to lie between flexor carpi radialis & palmaris longus tendons.
It enters the hand through the carpal tunnel, where it becomes:
1.Deep to flexor retinaculum
2.Superficial to flexor digitorum superficialis
After the median nerve leaves the cubital fossa , it enters the forearm.
The median nerve is considered as the main nerve of the anterior compartment of the forearm
Note
(It supplies all muscles of the anterior compartment of the forearm expect for flexor carpi ulnaris and medial half of the flexor digitorum profundus ,which are supplied by the ulnar nerve)It passes between the two heads of the pronator teres muscle
Note
(where it is separated from ulnar a. by the deep head of pronator teres)It descends between flexor digitorum superficialis above & flexor digitorum profundus below.
About 5 cm above wrist, it emerges from lateral border of flexor digitorum superficialis to lie between flexor carpi radialis & palmaris longus tendons.
It enters the hand through the carpal tunnel, where it becomes:
1.Deep to flexor retinaculum
2.Superficial to flexor digitorum superficialis
4. Hand
It enters the hand through the carpal tunnel , deep to the flexor retinaculum , along the nine tendons of the FDS , FDP , and FPL.
FDS: Flexor Digitorum Superficialis
FDP: Flexor Digitorum Profundus
FPL: Flexor Pollicis Longus
The median nerve ends at the distal border of the flexor retinaculum by dividing into lateral & medial divisions which also divide into palmar digital branches.
It gives motor nerve supply to:
1. Two and half thenar muscles
2. The first and second lumbricals
It also gives sensory nerve supply to:
1.Lateral two thirds of the palm of the hand
2.The sides of the lateral three and half fingers
3.The dorsum of the distal halves of the lateral three and half fingers
It enters the hand through the carpal tunnel , deep to the flexor retinaculum , along the nine tendons of the FDS , FDP , and FPL.
FDS: Flexor Digitorum Superficialis
FDP: Flexor Digitorum Profundus
FPL: Flexor Pollicis Longus
The median nerve ends at the distal border of the flexor retinaculum by dividing into lateral & medial divisions which also divide into palmar digital branches.
It gives motor nerve supply to:
1. Two and half thenar muscles
2. The first and second lumbricals
It also gives sensory nerve supply to:
1.Lateral two thirds of the palm of the hand
2.The sides of the lateral three and half fingers
3.The dorsum of the distal halves of the lateral three and half fingers
Branches
In the axilla
There is no branches .
In the arm
One vasomotor branch to the brachial artery.
In the forearm
Here it gives its main branches which include :
1- Articular branch : to the elbow joint ( arises in cubital fossa ).
2- Muscular branches : before it gives the anterior interosseous branch, it gives motor branches to the superficial group of muscles of the anterior compartment of the forearm.
It gives the nerve supply to the pronator teres m. usually at the elbow and enters the lateral border of the muscle .
It also sends some nerve fibers which pierces the superficial group of muscles ( which include FDS , FCR and palmaris longus).
3- Anterior interosseous branch : this nerve arises from the median nerve as the median nerve emerges between the two heads of the pronator teres muscle .
Then it runs on the anterior surface of the interosseous membrane and gives nerve supply to the lateral half of FDP.
It passes deep to and supply the pronator quadratus muscle .
It ends on the anterior surface of carpus by giving articular branches to the elbow and the inferior radioulnar joints .
4- Palmar cutaneous branch : It arises from the median nerve just proximal to the flexor retinaculum and passes over the flexor retinaculum to innervate the skin of the lateral part of the palm ( lateral two thirds of the palm ).
Then it runs on the anterior surface of the interosseous membrane and gives nerve supply to the lateral half of FDP
Note
(where the medial half is innervated by ulnar nerve ) It passes deep to and supply the pronator quadratus muscle .
It ends on the anterior surface of carpus by giving articular branches to the elbow and the inferior radioulnar joints .
4- Palmar cutaneous branch : It arises from the median nerve just proximal to the flexor retinaculum and passes over the flexor retinaculum to innervate the skin of the lateral part of the palm ( lateral two thirds of the palm ).
In the Hand
1- Recurrent ( muscular ) branch : it curves back around the distal border of the flexor retinaculum and lies about one fingerbreadth distal to the tubercle of the scaphoid bone . Here it innervates the muscles of the thenar compartment.
2- Palmar digital branches :
A. Lateral division : gives 3 palmar digital nerves, which supply 2 sides of thumb & lateral side of index.
The nerve to index also supplies first lumbrical muscle.
B. Medial division : gives 2 palmar digital nerves, which supply adjacent sides of (index, middle), (middle, ring) fingers.
Note(1) : the lateral one of these two nerves gives a branch to second lumbrical muscle.
Note(2) : the medial one these two nerves communicates with the palmar digital branch of ulnar nerve.
Note(3) :Palmar digital branches also give sensory nerve supply to the palmar surfaces , the sides and the dorsum of the distal phalanges of the lateral three and half fingers.
1- Recurrent ( muscular ) branch : it curves back around the distal border of the flexor retinaculum and lies about one fingerbreadth distal to the tubercle of the scaphoid bone . Here it innervates the muscles of the thenar compartment
Note
( flexor pollicis brevis , abductor pollicis brevis and opponens pollicis ) 2- Palmar digital branches :
A. Lateral division : gives 3 palmar digital nerves, which supply 2 sides of thumb & lateral side of index.
The nerve to index also supplies first lumbrical muscle.
B. Medial division : gives 2 palmar digital nerves, which supply adjacent sides of (index, middle), (middle, ring) fingers.
Note(1) : the lateral one of these two nerves gives a branch to second lumbrical muscle.
Note(2) : the medial one these two nerves communicates with the palmar digital branch of ulnar nerve.
Note(3) :Palmar digital branches also give sensory nerve supply to the palmar surfaces , the sides and the dorsum of the distal phalanges of the lateral three and half fingers.
Clinical notes
1. Median nerve injury at the elbow
It occurs when the median nerve is damaged at the elbow joint which causes the following symptoms :
1. Loss of flexion of the proximal interphalangeal joints of the first , second and third digits , and flexion of the fourth and fifth digits is weakened.
2. Loss of flexion of the distal interphalangeal joints of the second and the third digits but flexion of the fourth and fifth digits doesn’t become affected ( because the medial half of flexor digitorum profundus is innervated by the ulnar nerve ) .
3. The ability to flex the metacarpophalangeal joints of the second and third digits is affected , because the digital branches of the median nerve supply the first and second lumbricals thus when the person attempts to make a fist , the second and third fingers remain partially extended .
4. The function of the thenar muscles also is lost ( muscles which act at the base of the thumb) , Ape-like deformity which is the loss of the flexion & the opposition of thumb but the adduction of the thumb doesn’t become affected.
5. Loss of the forearm pronation (because of the paralysis of pronator teres and pronator quadratus muscles).
6. Loss of sensation at the lateral two-thirds of the palm and the lateral three and half fingers.
7- Weak flexion of wrist (because of the paralysis of flexor carpi radialis & palmaris longus).
2. Carpal Tunnel Syndrome
(damage at wrist)
Mechanism of injury
It occurs as a result of any lesion that reduces the size of the carpal tunnel or, more commonly , increases the size of some of the nine tendons.
As:
1. Inflammation of synovial sheaths
2. Fluid retention
3. Infection
4. Excessive exercise of the fingers may cause swelling of tendons and their synovial sheaths.
Also, dislocation of one of the carpals have the same effect .
Characteristic signs
1.The thenar eminence is wasted, due to atrophy of the thenar muscles.
2.If the patient tries to make a fist, only the little and ring fingers can flex completely.
This results in a characteristic shape of the hand, known as Hand of Benediction .Effect
1. The function of the thenar muscles also is lost ( muscles which act at the base of the thumb) , Ape-like deformity which is the loss of the flexion & the opposition of thumb but the adduction of the thumb doesn’t become affected.
2. Loss of sensation at the lateral two-thirds of palm and the lateral three and half fingers.
Characteristic signs
The hand is held in the same position as if it has been damaged at the elbow, but the forearm is unaffected (not supinated or adducted, wrist flexion it is likely unaffected, and also depending on the location of the lesion) .
References
References
1.Keith L. Moore , Arthur F. Dalley A. M. R. Agur; Moore clinically oriented anatomy 7thedition ;pp.723,724,729,733,735, 738-739,743,761,762,767,768,784-785,786,790-792,806,811, 812,813
2.Dr. Lawrence E. Wineski,PhD;SNELLIS CLINICAL ANATOMY BY REGIONS 10th edition;pp.239,285,291,294,339,342,343,344- 346,356-361,466
3. Median Nerve: Anatomy, Origin, Course, Function, Clinical Importance; Physiotherapy_Clinic; Mobile Physiotherapy Clinic; https://mobilephysiotherapyclinic.in/median-nerve/
4. Median nerve; Shahab Shahid ,MBBS;Kenhub; https://www.kenhub.com/en/library/anatomy/the-median- nerve
5. The Median Nerve; Oliver Jones; teachmeanatomy; https://teachmeanatomy.info/upper-limb/nerves/median- nerve/
6. Anatomy, Shoulder and Upper Limb, Median Nerve; Kelly A. Murphy, Daphne Morrisonponce; National Library of Medicine; https://www.ncbi.nlm.nih.gov/books/NBK448084/
1.Keith L. Moore , Arthur F. Dalley A. M. R. Agur; Moore clinically oriented anatomy 7thedition ;pp.723,724,729,733,735, 738-739,743,761,762,767,768,784-785,786,790-792,806,811, 812,813
2.Dr. Lawrence E. Wineski,PhD;SNELLIS CLINICAL ANATOMY BY REGIONS 10th edition;pp.239,285,291,294,339,342,343,344- 346,356-361,466
3. Median Nerve: Anatomy, Origin, Course, Function, Clinical Importance; Physiotherapy_Clinic; Mobile Physiotherapy Clinic; https://mobilephysiotherapyclinic.in/median-nerve/
4. Median nerve; Shahab Shahid ,MBBS;Kenhub; https://www.kenhub.com/en/library/anatomy/the-median- nerve
5. The Median Nerve; Oliver Jones; teachmeanatomy; https://teachmeanatomy.info/upper-limb/nerves/median- nerve/
6. Anatomy, Shoulder and Upper Limb, Median Nerve; Kelly A. Murphy, Daphne Morrisonponce; National Library of Medicine; https://www.ncbi.nlm.nih.gov/books/NBK448084/