Pectoralis Major (P.Mj)
By : Fahad Al-BakNaming: -
/PEK-to-ra-lis MAY-jor/
The name is from Pectoral (meaning chest) and major refers to its size (also means that there is a minor one [smaller]).
The name is from Pectoral (meaning chest) and major refers to its size (also means that there is a minor one [smaller]).
General: -
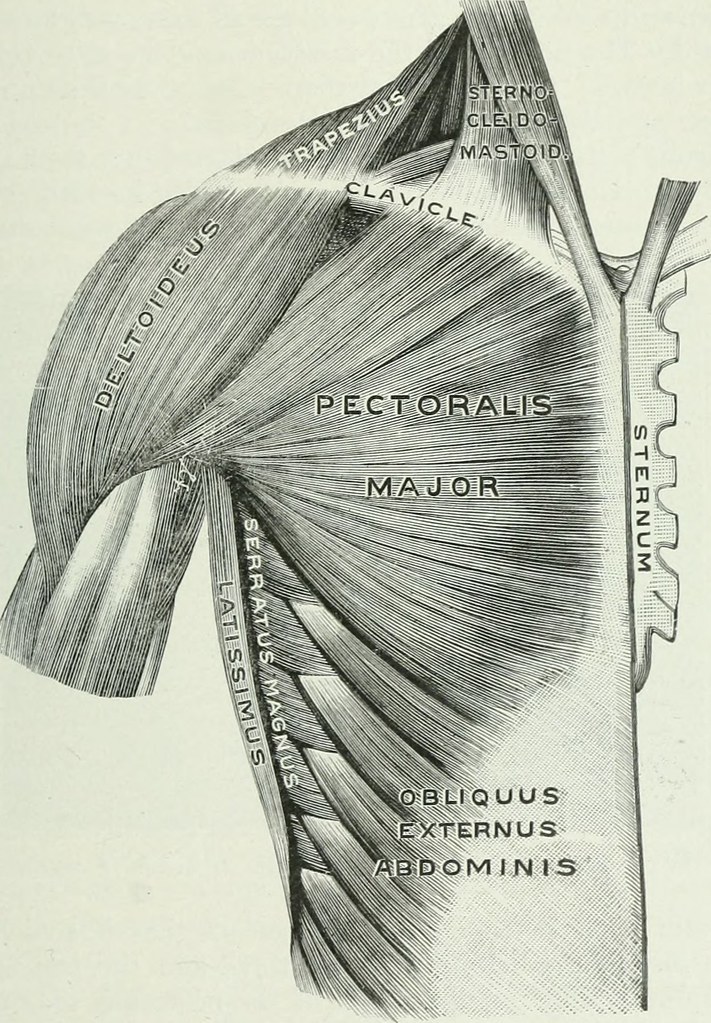
The pectoralis major is a triangular shaped thick muscle on the upper anterior part of the chest (the thoracic wall) crossing over to the axilla and the arm, it is a superficial muscle thus it is the muscle that give the upper chest it signatures shape. It belongs to the Muscles of the Glenohumeral Joint.
Supply: -
-The blood supply for this muscle is The Pectoral branches of the Thoracoacromial Trunk (a branch of the Axillary Artery and the Posterior Intercostal Arteries (branches of the Aorta) and the Lateral Thoracic Artery (a branch of the Axillary Artery).
-The P.Mj nerve supply comes from the Medial and Lateral Pectoral Nerves (C5, C6, C7, C8, T1).

Origin & Insertion: -
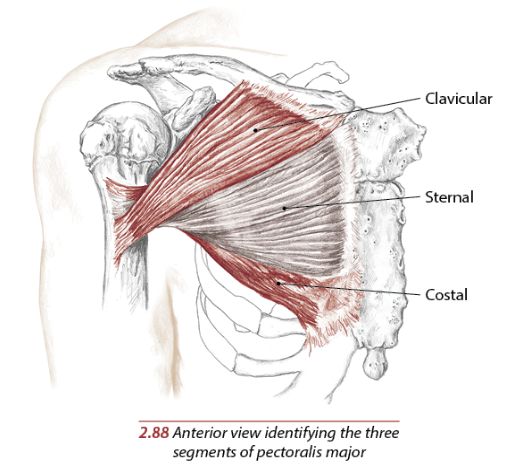
-Origin (Medial Clavicle, Sternum, the Costal Cartilages of Ribs One through Seven and the aponeurosis of the external abdominal oblique): It has clavicular and sternocostal parts, which may be separated by a groove, although they are usually continuous with each other. The smaller, clavicular attachment is from the medial half of the anterior surface of the clavicle; the larger, sternocostal attachment comes from the anterior surface of the manubrium and body of the sternum, the anterior aspects of the upper six costal cartilages, the anterior part of the sixth rib as well as the aponeurosis of the external oblique muscle of the abdomen.
-Insertion (Lateral Lip of the Bicipital Groove of the Humerus): From this large medial attachment, the muscle narrows and inserts via a laminated tendon into the lateral lip of the intertubercular groove of the humerus. The anterior lamina, which is the clavicular part of the muscle, runs to the lower part of the humeral attachment. The sternocostal part forms the posterior lamina, which passes upwards behind the anterior lamina to the upper part of the attachment to the humerus. In this way the tendon comes to resemble a U in cross-section. The posterior part blends with the shoulder joint capsule, while the anterior, clavicular fibers blend with the attachment of deltoid.
Motion & Action: -
( Adducts the arm at shoulder, Medially rotates the arm at the shoulder, Flexes the arm at the shoulder and Extends the arm at the shoulder joint )
Pectoralis major as a whole is a strong adductor and medial rotator of the humerus at the shoulder joint. In addition, the clavicular part can flex the humerus to the horizontal, while the sternocostal fibers, because of their direction, can extend the flexed humerus, particularly against resistance in the anatomical position.
With the humerus fixed, as in holding on to a bed, table or chair back, pectoralis major pulls on the upper ribs to assist inspiration during respiratory distress.
Pectoralis major is one of the major climbing muscles, so that if the arms are fixed above the head, the power of the muscle can be used to pull the trunk upwards.
It is helps in this activity by latissimus dorsi. In pushing, punching and throwing movements, pectoralis major acts to move the humerus forcefully forwards, while serratus anterior and pectoralis minor simultaneously protract the pectoral girdle. In exercises, such as the ‘press-up’, pectoralis major contracts concentrically on the upward movement raising the body and eccentrically on the downward action when lowering the body.
Pectoralis major as a whole is a strong adductor and medial rotator of the humerus at the shoulder joint. In addition, the clavicular part can flex the humerus to the horizontal, while the sternocostal fibers, because of their direction, can extend the flexed humerus, particularly against resistance in the anatomical position.
With the humerus fixed, as in holding on to a bed, table or chair back, pectoralis major pulls on the upper ribs to assist inspiration during respiratory distress.
Pectoralis major is one of the major climbing muscles, so that if the arms are fixed above the head, the power of the muscle can be used to pull the trunk upwards.
It is helps in this activity by latissimus dorsi. In pushing, punching and throwing movements, pectoralis major acts to move the humerus forcefully forwards, while serratus anterior and pectoralis minor simultaneously protract the pectoral girdle. In exercises, such as the ‘press-up’, pectoralis major contracts concentrically on the upward movement raising the body and eccentrically on the downward action when lowering the body.

In The Field Notes: -
Testing the Pectoralis Major function: The clavicular part of pectoralis major can be readily tested if the arm is flexed to 60 degrees and held against downward pressure. The sternocostal part is best tested if this same position is maintained against an upward pressure. The integrity of the muscle can be fully tested by adduction of the arm against resistance.
Clinical Note: -
-Damage of the pectoralis major: The injury of the P.Mj is rare and tendon tears occurring almost exclusively in males from 20 to 40 years old, and around 50% of these are sustained during weight-bearing exercises such as the bench press when the arm under load is in extension and external rotation. Examination of a pectoralis major rupture will see swelling, hematoma, medialization of the muscle bed, tenderness along the humeral insertion, and along the axilla. These signs are not stable and may develop rapidly or over a period of weeks. Investigation of potential pectoral injury centers around clinical history and examination and radiology. Chest x-ray can rule out bony injury (avulsion occurring in 2% to 5% of cases), and ultrasound and MRI are well known to be able to diagnose and characterize tears.
The majority of tears are conservatively managed via analgesia and sling immobilization in the adducted and internally rotated position. The patient may gradually increase action from 2 to 6 weeks. Light resistance activities can then be acted from 6 to 8 weeks, and full return to resistance activity is possible at 3 to 5 months. However, in cases of complete tears or in the young and athletic population, operative repair is a better choice and is ideally performed within 6 weeks of injury. For the young and those involved in sports, surgical repair is the most appropriate way to regain the most strength, mobility, and function.

Relations: -
The pectoralis major is superficial in the chest.
The pectoralis minor and the subclavius, as well as the proximal attachments of the coracobrachialis and the short and long heads of the biceps brachii, are deep to the pectoralis major.
Lateral to the clavicular head of the pectoralis major is the anterior deltoid.
The pectoralis major is located within the superficial front arm line and front functional line myofascial meridians.
The pectoralis minor and the subclavius, as well as the proximal attachments of the coracobrachialis and the short and long heads of the biceps brachii, are deep to the pectoralis major.
Lateral to the clavicular head of the pectoralis major is the anterior deltoid.
The pectoralis major is located within the superficial front arm line and front functional line myofascial meridians.
Sources: -
- Joseph E Muscolino - The Muscular System Manual: The Skeletal Muscles of the Human Body 4th edition Book (125-127).
-Nigel Palastanga & Roger Soames Anatomy and Human Movement Structure and Function 6th edition (61-62).
- Anatomy, Thorax, Pectoralis Major by Francesca Solari; Bracken Burns – NLH
-Nigel Palastanga & Roger Soames Anatomy and Human Movement Structure and Function 6th edition (61-62).
- Anatomy, Thorax, Pectoralis Major by Francesca Solari; Bracken Burns – NLH